|
|
Illustrated text with links to cases |
|
|
|
Illustrated text with links to cases |
|
| This page in Portuguese | Site in Portuguese | English homepage |
| PILOCYTIC
ASTROCYTOMA
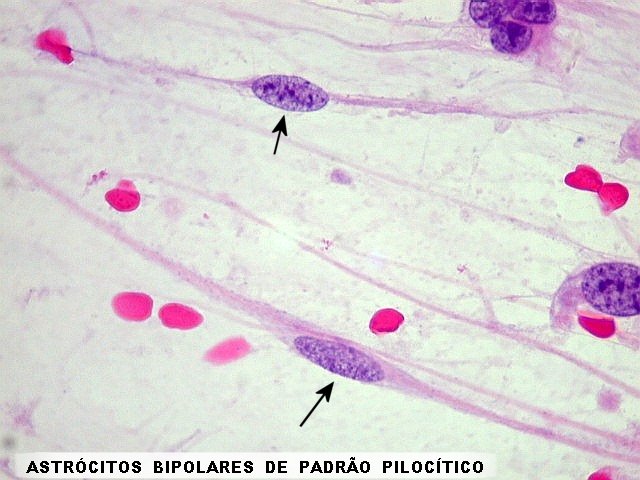
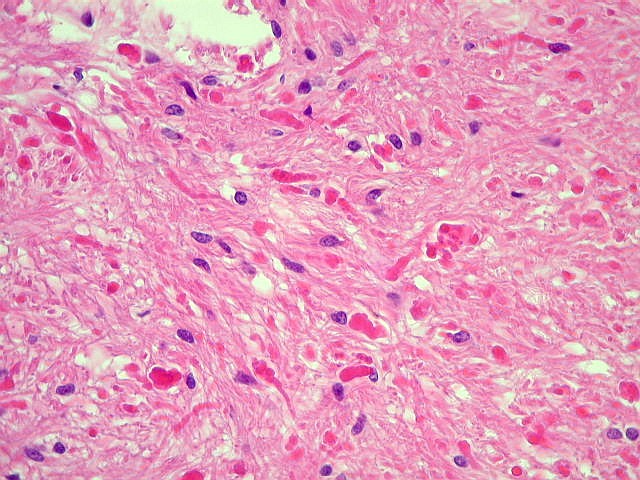
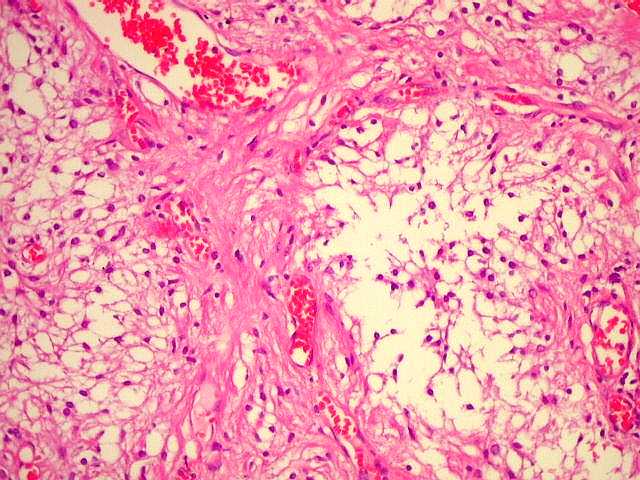
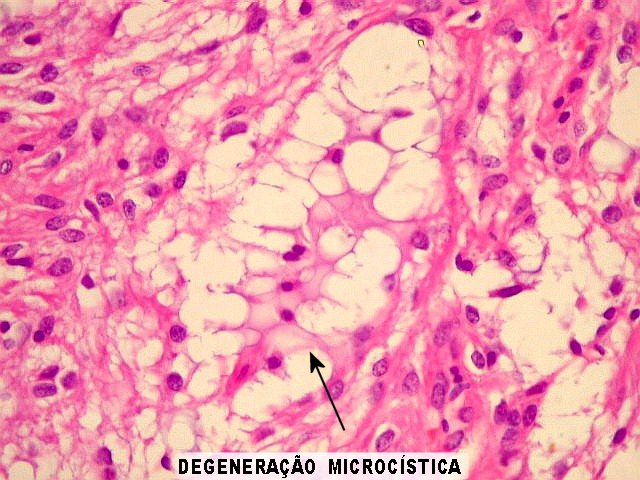
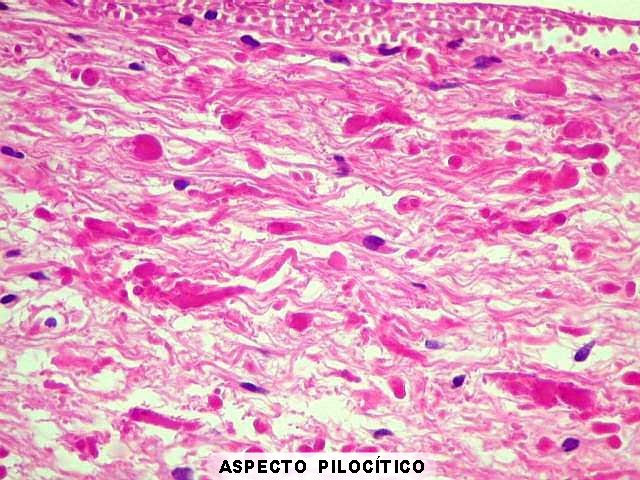
Definition. A well delimited, often cystic astrocytic tumor composed of variable proportions of compact (pilocytic) and loose (protoplasmatic) tissue which are frequently found together in the same specimen (so called biphasic pattern). Pilocytic or piloid areas are characterized by elongated bipolar cells with slender processes in parallel arrangement. Hyaline inclusions known as Rosenthal fibers are common. Protoplasmatic astrocytes populate the loose areas. They have multiple short processes leaving spaces or microcysts containing basophilic fluid. Most tumors grow slowly and non invasively and are accordingly classified was WHO grade I. It should
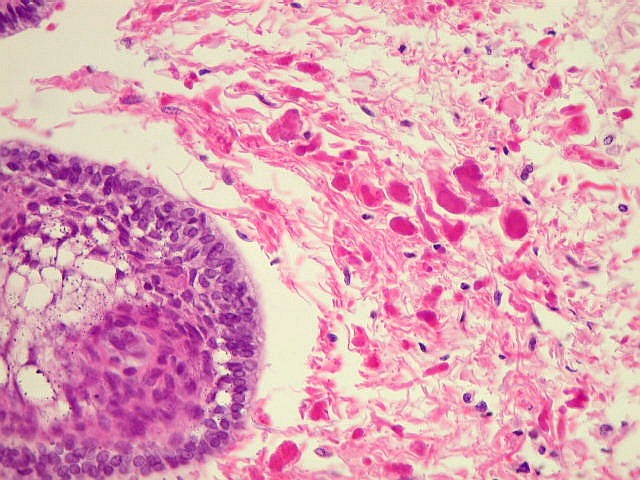
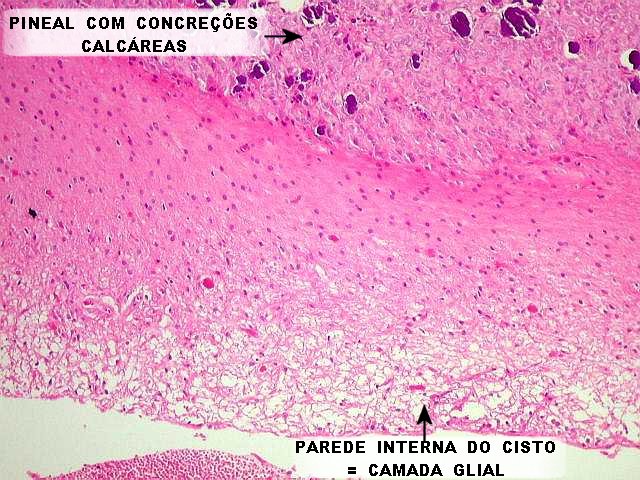
be noted that piloid tissue also occurs in long standing gliosis, particularly
around such chronic lesions as craniopharyngiomas
and pineal cysts, and is therefore not exclusive
nor diagnostic of pilocytic astrocytomas. Conversely, lack of pilocytic
tissue does not rule out the diagnosis.
Age. Pilocytic astrocytomas occur mostly in the two earlier decades of life (over 75% of cases) with a peak between 8 and 13 years. Exceptions may be found in later life up to the 8th decade, of which we boast two cases of our own (1) (2). Pilocytic astrocytomas make up 85% of cerebellar and 10% of cerebral astrocytomas. Neurofibromatosis type 1 (NF1) is an important predisposing factor, particularly to optic nerve gliomas, which in that case may be bilateral. Sites. Commonest are (see table for pilocytic astrocytomas by topography) 1) Cerebellum,
predominantly the hemispheres
Bulky tumors
in the basal region of the cerebral hemispheres may defy precise definition
of the site of origin.
Clinical findings. Cerebellar tumors may cause ataxia and intracranial hypertension (headache, nausea, vomiting, papilledema) due to fourth ventricle obstruction. Elevated intracranial pressure may in time cause blindness through optic nerve ischemia, as CSF is forced into the subarachnoid space around the nerve, contained by a sheath of dura mater. Many patients are in the pediatric age and may not complain of visual loss. Optic nerve gliomas lead to drop in visual acuity and eventually blindness. Large tumors may cause proptosis. Again, as tumors grow extremely slowly, visual complaints may be minor or absent. Tumors of the optic chiasm and pathways, may be accompanied, besides visual loss, by signs of hypothalamic or pituitary dysfunction, such as precocious puberty, hypogonadism, obesity and diabetes insipidus. Tumors obliterating the third ventricle may produce hydrocephalus. Brainstem tumors are mostly situated in the mesencephalic tegmentum (region of the quadrigeminal plate) where they cause early acqueductal obstruction and hydrocephalus. By contrast, diffuse astrocytomas more commonly affect the basis pontis and grow in infiltrative fashion among the axons, leading to so called 'hypertrophy' of the pons. Thalamic tumors and those at the base of the cerebral hemispheres may present with hemiparesis through compression of the internal capsule, or hydrocephalus due to third ventricle obstruction. Tumors situated elsewhere
in the cerebral hemispheres may cause localized deficits,
mass effect, particularly when associated
with cysts, and are associated with epilepsy (of which we have three
cases of our own (1)(2)(3).
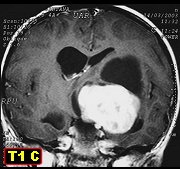
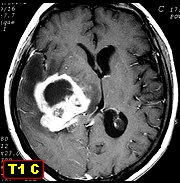
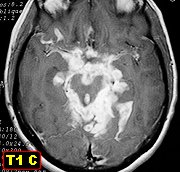
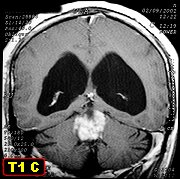
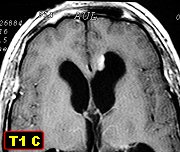
Neuroimaging. Click for exemples and text. Basic elements for diagnosis are well defined tumor limits, diffuse contrast enhancement and a relative lack of peritumoral edema, the latter attributed mainly to slow growth. Cysts, single or multiple, are often present. Contrast enhancement of the cyst wall argues in favor of the cyst being part of the tumor. On the other hand, diffuse astrocytomas of the cerebral hemispheres and brain stem are poorly delimited, non enhancing masses, and only take up contrast when anaplasia sets in. Other tumor entities sharing neuroimaging features with pilocytic astrocytomas are xanthoastrocytomas, gangliogliomas and ependymomas, all of which can only be distinguished from one another through histopathological examination. Macroscopical appearances. Optic
nerve gliomas characteristically grow along the nerve
(in fact not a real nerve but a tract of white matter) causing spindle
or pear shaped enlargement. The tumor remains confined by the dural sheath
surrounding the nerve. On section, the enlarged nerve appears whitish
and firm. A collar of greyish tissue corresponds to infiltrated subarachnoid
space with desmoplastic reaction (production of reticulin fibers in response
to tumoral invasion).
At other locations, including the cerebellum, pilocytic astrocytomas form well delimited, firm, pinkish to white masses, which may appear homogeneous or associated with cysts. A mural nodule in a cyst wall is typical. Microscopy. Classical pilocytic astrocytomas associate two histological appearances (biphasic pattern).
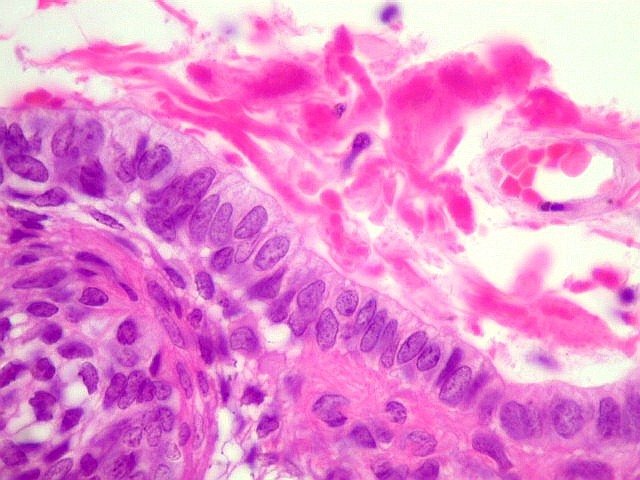
This biphasic pattern may be lacking, and the sample may contain only one type of tissue. The diagnosis must thus find support in other data such as age, location and neuroimaging studies. In typical
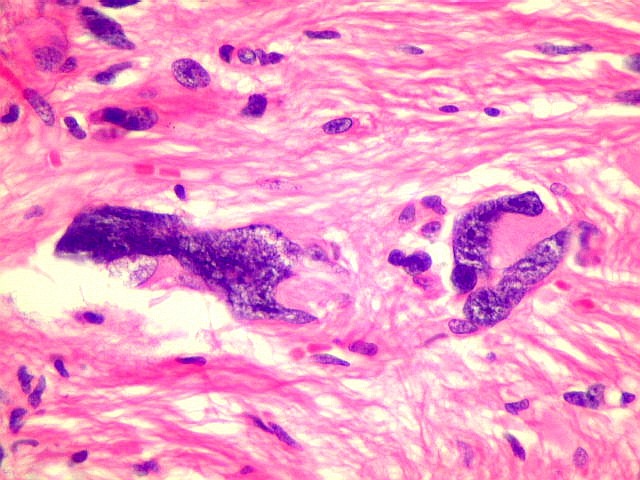
pilocytic astrocytomas, nuclei are round to oval with finely stipled chromatin.
However, nuclear atypia may occur, sometimes
reaching bizarre proportions. Such changes are attributed to degenerative
phenomena and are particularly striking in long standing tumors. They should
not be viewed as evidence of anaplasia or aggressive behavior. Grossly
atypical nuclei are usually negative for the Ki-67 (MIB1) proliferation
marker.
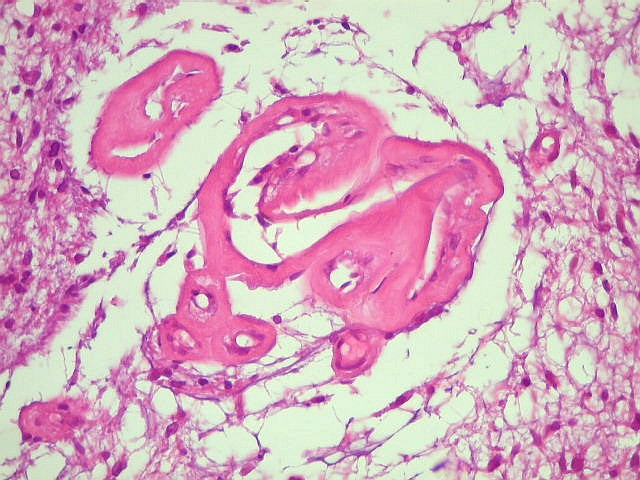
Thickened hyalinized vessels are another feature suggestive of tumor senescence, as are hemosiderin deposits and chronic inflammatory infiltrate. Calcifications occur in only a minority of cases and are mostly inconspicuous. Subarachnoid extension
is a relatively common finding, particularly in cerebellar astrocytomas
which grow amid the foliae, and in optic nerve gliomas. Again, these
invasive features do not anticipate aggressiveness or distant spread through
CSF pathways.
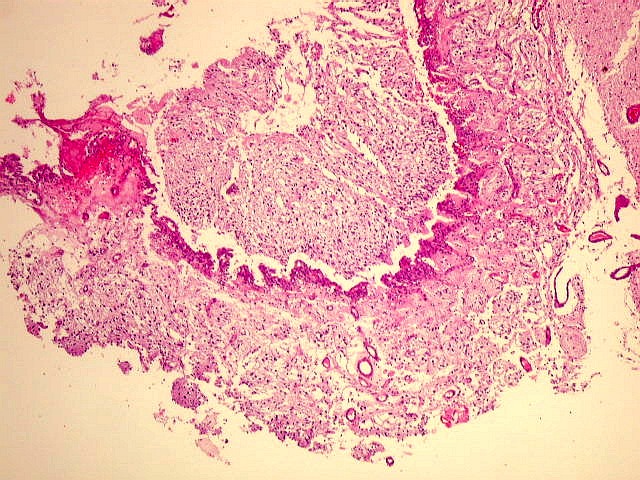
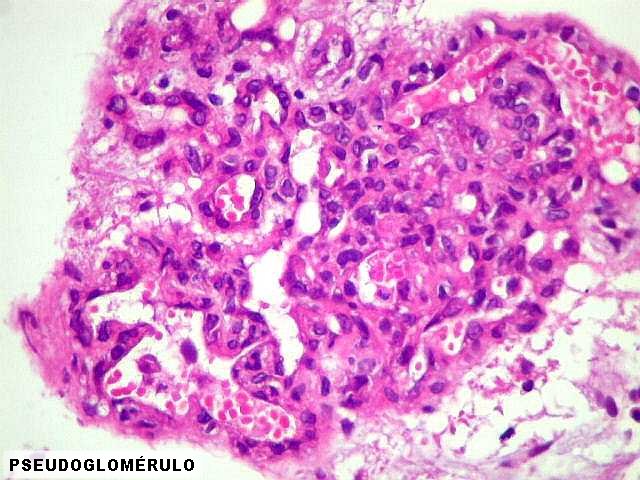
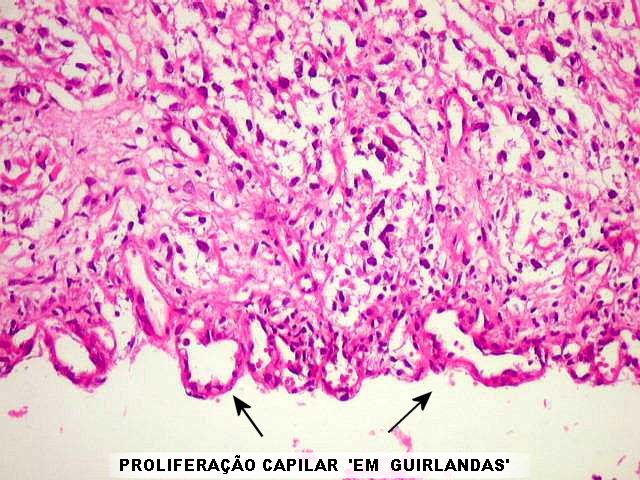
Vascular proliferation
is another important feature of pilocytic astrocytomas and may be prominent
enough to rival the pseudoglomeruli of glioblastoma multiforme. Care is
therefore essential not no overgrade an otherwise typical pilocytic astrocytoma
on account of its proliferated vessels.
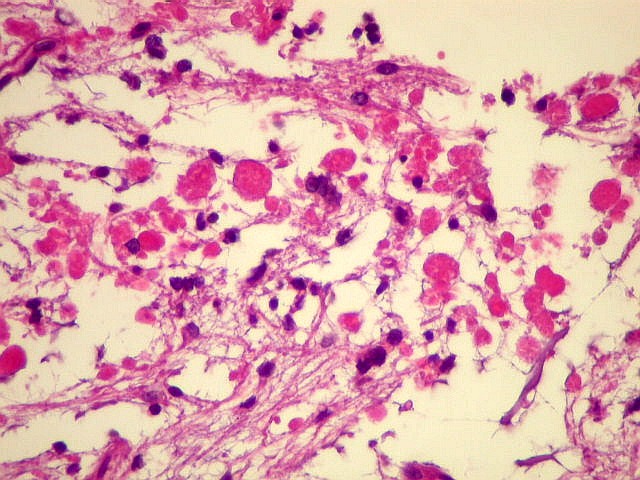
Necrosis is seen in up to 8% of pilocytic astrocytomas and is usually infarct-like, affecting larger areas. Small areas of necrosis with pseudopalisading as seen in glioblastomas are not a feature. Hyaline bodies (also
known as hyaline granular bodies or eosinophilic granular bodies) are droplets
of proteic material among tumor cells common in slow growing tumors
such as pilocytic astrocytomas, gangliogliomas and xanthoastrocytomas.
Their presence attests to the relatively benignity of the neoplasm and
guards against a diagnosis of diffuse astrocytoma. In pilocytic astrocytomas
they are more usually found in protoplasmatic areas, whereas Rosenthal
fibers are more abundant in piloid areas.
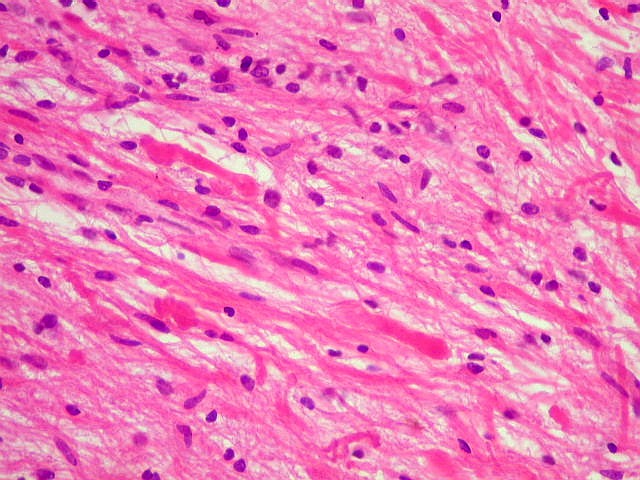
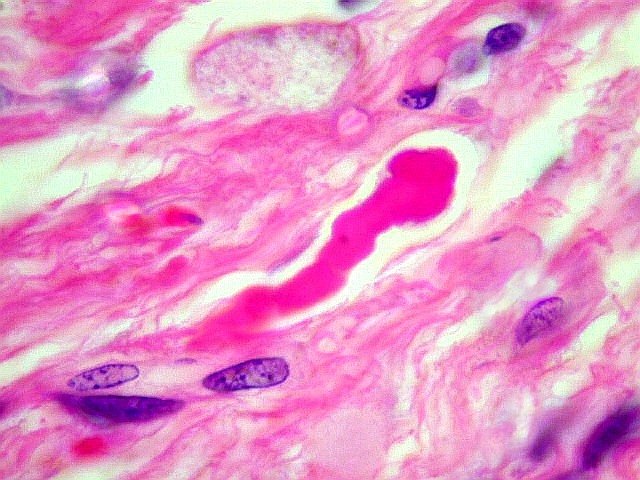
Rosenthal
fibers are elongated hyaline structures characteristically
shaped as a carrot or sausage, and are found largely in pilocytic tissue.
Some have a beaded appearance. They occur as electron-dense protein
deposits within the processes of neoplastic cells and are not made up of
GFAP but of the lens protein a-B
crystallin. When found in a tumor they strongly argue in favor of
pilocytic astrocytoma or a ganglioglioma with pilocytic component. Their
absence does not exclude either diagnosis. It must be borne in mind
that Rosenthal fibers also occur in long standing areas of gliosis such
as around craniopharyngiomas, and this should be taken into account when
examining tissue from sites where both tumors occur, namely the hypothalamic
region.
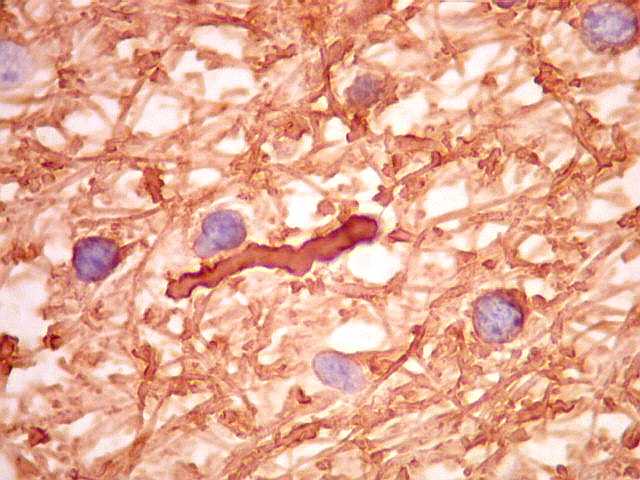
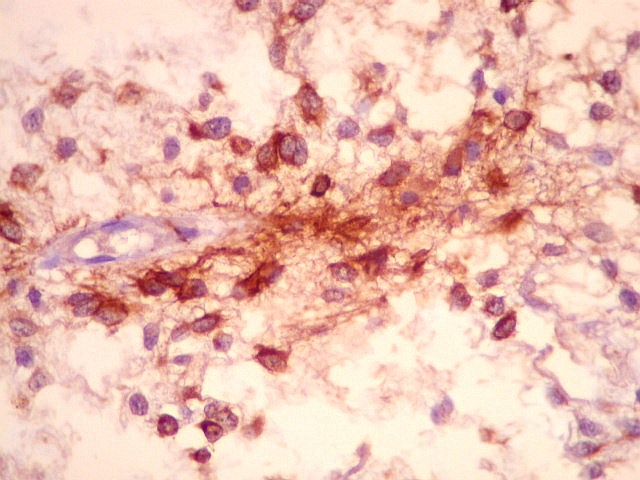
Immunohistochemistry.
Neoplastic astrocytes are positive for GFAP, more strongly so in
piloid areas. In protoplasmatic tissue positivity is variable. Rosenthal
fibers are negative for GFAP, except at the periphery, where they may show
a GFAP coat. Hyaline granular bodies are positive for a1-antitrypsin
e a1-antichymotrypsin.
Labelling by Ki-67 (MIB-1) is usually low in tumor cells. In the literature,
higher indices have not been indicative of worse prognosis. Labeled nuclei
may be more numerous in endothelial cells of hyperplastic capillaries than
in the tumor cells themselves.
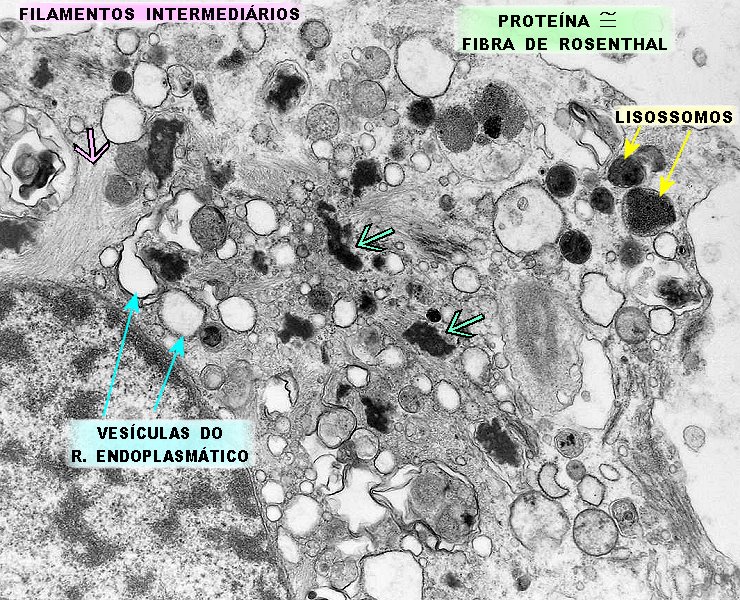
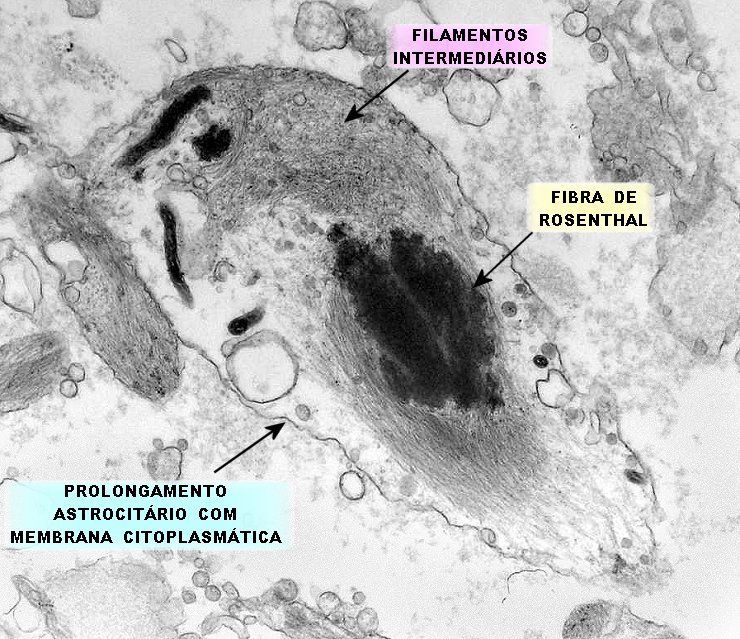
Eletron Microscopy .
Pilocytic astrocytes are rich in cytoplasmic organelles, such as rough
and smooth endoplasmic reticulum, mitochondria and lysosomes. There
are also variable quantities of intermediate filaments, which are mainly
GFAP and vimentin. Intermingled with these there are often irregular
electron dense deposits of protein corresponding to Rosenthal fibers. These
are observed both in the cell body and processes. Click
for more details.
Grading and prognosis.
Pilocytic astrocytomas are and remain, with few exceptions, WHO grade I.
Histological features with ominous significance in diffuse astrocytomas
(WHO grades II to IV)
Cerebellar pilocytic astrocytomas carry the best prognosis because they are more amenable to total surgical ressection. 5-year survival approaches 100%. Partial ressection may be followed by recurrences, more often through cyst expansion than tumor regrowth. Optic nerve tumors usually grow very slowly and may even stabilize or regress spontaneously, particularly in NF1. Tumors of the optic chiasm and hypothalamic region progress inexorably, as complete ressection is out of the question. Cyst formation within the tumor may contribute more to the mass effect than growth of the neoplasm itself. Tumors situated
superficially in the cerebral hemispheres may be cured by surgery. On the
other hand, deep seated lesions in the thalamus or basal ganglia may expand
swiftly and/or recur shortly after
surgical ablation. We draw attention to a particularly aggressive example
of presumed cerebellar origin which disseminated widely to the basal leptomeninges.
Dissemination through
CSF pathways. It is well
known that pilocytic astrocytomas, though rarely, may seed distant sites
via the CSF, even before the primary tumor announces itself. This behavior
is more commonly described with hypothalamic primaries. Proliferative
indices in these cases may be high or low. We have a case
of a cerebellar tumor with implants in the third and lateral ventricles,
in which the original lesion showed the bland biphasic pattern of slow
growing pilocytic astrocytomas. After three years there was no recurrence
of the original lesion and little growth at the secondary sites.
Malignant transformation. Pilocytic astrocytomas are remarkably stable and keep their WHO grade I status for years or decades. Increased cellularity, nuclear atypia and scanty mitoses (less than 1-2 per 10 high power fields) herald no change in prognosis. The rare examples of pilocytic astrocytoma undergoing malignant change occur mostly after radiotherapy. These should be termed anaplastic pilocytic astrocytoma rather than glioblastoma multiforme, as the outcome is hardly as grim as with diffuse astrocytomas. Differential diagnosis.
The first point is to rule out non neoplastic, long standing gliosis as
often found around craniopharyngiomas in the
hypothalamic region and hemangioblastomas of cerebellum. Difficulty can
also arise in gliosis associated with vascular malformations, of which
we had a case in the optic nerve.
Neuroimaging studies may be of great help in deciding such issues.
Tumors mimicking pilocytic astrocytoma in imaging studies are ganglioglioma and pleomorphic xanthoastrocytoma. Both can have histological features in common with the pilocytic astrocytomas, such as hyaline granular bodies. Rosenthal fibers may be a feature of gangliogliomas with pilocytic component, but not of xanthoastrocytoma. Gangliogliomas show dysmorphic, irregularly distributed neurons, which may be highlighted with appropriate immunohistochemical techniques. Xanthoastrocytomas are usually more cellular, more pleomorphic, may show fascicular architecture, reticulin fibers and sometimes xanthomatous astrocytes. Microcysts are not found. Most important from the prognostic point of view is to exclude diffuse astrocytomas, a task greatly facilitated by neuroimaging. Low grade astrocytomas are poorly delimited, non enhancing and cysts are uncommon. High grade tumors may show scattered foci of contrast enhancement or annular impregnation around a necrotic center. They are often accompanied by mass effect and white matter edema far greater than the usual for pilocytic astrocytomas. Main sources:
|
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| This page in Portuguese | Site in Portuguese | English homepage |
| Neuropatologia
- Graduação |
Neuropatologia -
Casos Complementares |
Neuroimagem
- Graduação |
Neuroimagem -
Casos Complementares |
Correlação
Neuropatologia - Neuroimagem |